Written By: Ki Lov3 (Chanele)
Edited by: Toni the Editor
Date: October 15, 2025
Or listen to this article FREE on our Spotify podcast 🎙️🌐https://spotify.link/fgfMGA3qvXb
Hi, my name is Chanele. I am a writer under the pen name Ki Lov3. Those who know me or follow my works online have noticed that I do not share my personal and private information online or in person; especially about my mental health struggles. In general my online “persona” is all business, encouraging those to pay it forward – by providing educational information to those who want it. If you follow me or any of my projects online, even the majority of my books are written with the intention of helping and caring about others. Don’t feel left out, I am the same way to those in my everyday life. Go ahead and look me up. You won’t find anything about my personal struggles, I will wait (🥱 As I said nothing). This entire project is going to be just as surprising to you as the people closest to me. Yet, at the ripe older and wiser version of me at 46 years old, I have the need, want, and platforms to express my true and authentic self mental health struggles in a very transparent way.
Spotify podcast episode
Why now is probably what you are asking?
I kept my mental health issues private for the majority of my life, not because I was ashamed but rather because they were intimate. I decided to only share them with those I trusted because they were a part of who I was. Recently, I was deprived of that option. My most private information, including my medical and mental health records was made public when my wife and I fell victim to identity theft and hacking starting in May 2025. It felt as if those pages from my diary had been handed to the world without my permission.
The experience reminds me of what it’s like to be outed as gay before you’re ready. Even now, the majority of civil society has collectively decided, ripping someone of the closet is part of today’s “Cancel Culture.”
Coming out or sharing personal sensitive information should be a moment of self-awareness and authenticity, and so should sharing one’s mental health journey. Being part of the LGBTQ community can attest to the damage it inflicts on a person’s life and mental health. Both are stories about identity, vulnerability, and truth; they deserve to be told in our own words. I know sometimes when viewing someone from behind the screens, people tend to see them as an object or brand with no rights or emotions. I am here to say, someone’s personal mental health status isn’t to be toyed with, keep in mind behind that profile is a real human with real emotions. What happened to myself and my wife is not only immoral but also illegal.
So now I’ve decided to speak openly. Not because I wanted to, but because many have seen my information on paper and created their own narrative spin to it. I now deserve to have a day in explaining my OWN life story. As well as, this experience has shown me how much ignorance and misinformation there still is in regards to certain mental illnesses. Yet, I no longer have the right to remain silent and at least be able to explain what the experience does to the human psyche, in an attempt to protect others’ privacy and mental health struggles be THEIRS. Since my story has already been taken and shared with the world, I will reclaim it and tell it in my own voice, with honesty, courage, and purpose.
The following is a scripted podcast to create a healthy space to explain that we all aren’t the same when it comes to my most vulnerable status. Yes, my name is Chanele, and I am diagnosed with mental health illnesses. One being Agoraphobia, and yes, I am a real person with real emotions and fears, like each of you reading and listening to this. To be completely transparent and authentic, I have been diagnosed with multiple disabilities but what I am discussing in this piece is,”bouts of Agoraphobia.” Which, I was diagnosed with after a lot of traumatic events and unfortunate situations. This has also resulted in also being diagnosed with Anxiety with panic attacks and PTSD to name a few, unfortunately there are more diagnoses because life has really punched me in the gut 😢.
Unlike your normal feed you scroll through, my life hasn’t been rainbows 🌈 and butterflies 🦋as we all try to portray on social media. Why? Well influencers aren’t born out of heartache, doom and gloom or pain. It isn’t a brand or online friend you want to have that always post about the negative things in their life. That just isn’t the society we live in online or in person. I have learned the hard way that if you share a vulnerability it will be weaponized against you as soon as that other person doesn’t get an answer they wanted or anything else they want. I will say 💒🫶🙏it again for the people in the back, I have been on my #NoNewFriendsSummer for over 10 years. And if you never experienced this:
Good for you!😉
What is your secret?
Seriously, what is it???? Inbox me 📩
Yes, I am super jealous because you have lived a charmed life.💔🥹
Why now is probably what you are asking?
I kept my mental health issues private for the majority of my life, not because I was ashamed but rather because they were intimate. I decided to only share them with those I trusted because they were a part of who I was. Recently, I was deprived of that option. My most private information, including my medical and mental health records was made public when my wife and I fell victim to identity theft and hacking starting in May 2025. It felt as if those pages from my diary had been handed to the world without my permission.
The experience reminds me of what it’s like to be outed as gay before you’re ready. Even now, the majority of civil society has collectively decided, ripping someone of the closet is part of today’s “Cancel Culture.”
Coming out or sharing personal sensitive information should be a moment of self-awareness and authenticity, and so should sharing one’s mental health journey. Being part of the LGBTQ community can attest to the damage it inflicts on a person’s life and mental health. Both are stories about identity, vulnerability, and truth; they deserve to be told in our own words. I know sometimes when viewing someone from behind the screens, people tend to see them as an object or brand with no rights or emotions. I am here to say, someone’s personal mental health status isn’t to be toyed with, keep in mind behind that profile is a real human with real emotions. What happened to myself and my wife is not only immoral but also illegal.
So now I’ve decided to speak openly. Not because I wanted to, but because many have seen my information on paper and created their own narrative spin to it. I now deserve to have a day in explaining my OWN life story. As well as, this experience has shown me how much ignorance and misinformation there still is in regards to certain mental illnesses. Yet, I no longer have the right to remain silent and at least be able to explain what the experience does to the human psyche, in an attempt to protect others’ privacy and mental health struggles be THEIRS. Since my story has already been taken and shared with the world, I will reclaim it and tell it in my own voice, with honesty, courage, and purpose.
The following is a scripted podcast to create a healthy space to explain that we all aren’t the same when it comes to my most vulnerable status. Yes, my name is Chanele, and I am diagnosed with mental health illnesses. One being Agoraphobia, and yes, I am a real person with real emotions and fears, like each of you reading and listening to this. To be completely transparent and authentic, I have been diagnosed with multiple disabilities but what I am discussing in this piece is,”bouts of Agoraphobia.” Which, I was diagnosed with after a lot of traumatic events and unfortunate situations. This has also resulted in also being diagnosed with Anxiety with panic attacks and PTSD to name a few, unfortunately there are more diagnoses because life has really punched me in the gut 😢.
Unlike your normal feed you scroll through, my life hasn’t been rainbows 🌈 and butterflies 🦋as we all try to portray on social media. Why? Well influencers aren’t born out of heartache, doom and gloom or pain. It isn’t a brand or online friend you want to have that always post about the negative things in their life. That just isn’t the society we live in online or in person. I have learned the hard way that if you share a vulnerability it will be weaponized against you as soon as that other person doesn’t get an answer they wanted or anything else they want. I will say 💒🫶🙏it again for the people in the back, I have been on my #NoNewFriendsSummer for over 10 years. And if you never experienced this:
Good for you!😉
What is your secret?
Seriously, what is it???? Inbox me 📩
Yes, I am super jealous because you have lived a charmed life.💔🥹
It is a diagnosis that most of us live independently and not needing to be in a facility kept guarded, all out of paranoia and fear of the myths, stereotypes and discrimination swaying people’s minds without even knowing them. “As I say, it isn’t paranoia if it is true.” This fear of people taking away our rights, the way we choose to live and taking over our financial situation, by making themselves our payee and guardian. Unfortunately, there are many predators looking to take advantage of us, especially when Social Security Disability Income is involved. Between the predators, opportunists, and overall haters, we have been driven into the dark corners of society.
In recent news, 60 year old former celebrity talk show host Wendy Williams is a pure and very public example of this very thing happening. watch Access Hollywood video about Wendy Williams here 2/2025 update This is why most of us with “invisible disabilities” try our best to keep the secret and fit into everyday living. Yet, another driving force in writing my story is because the rest of the disabled community that isn’t able to hide or keep the secret– for example, someone in a wheelchair, a blind person or amputee, doesn’t have the luxury to even attempt to fit in without judgement, stereotypes, and everyday discrimination before they even open their mouth. Not to say there hasn’t been progressive improvement over the years (thank you 🙏 American Disability Association and AARP👴👵 with ensuring legislation ⚖️laws and mandates have been put in place to shield us from the ridicule and discrimination).
Another comparison to my experience of having my personal mental health records exposed is similar to the issues I’ve written about regarding colorism within the Black community. Those with darker skin tones ✊🏾 understand this struggle all too well. For those unfamiliar, colorism refers to the bias or preference for lighter skin tones within communities of color, a painful reality rooted in systemic racism and social conditioning. It’s the idea that someone might be seen as “more acceptable” or “passing” because of lighter skin.
I encourage everyone, especially women of all backgrounds to read and reflect on those articles. Understanding these internalized struggles helps us all build more empathy and unity.
Wendy Williams update
As an update of the former celebrity talk show host as of February 2025, she still doesn’t have her own guardianship. Yet, in January she was just released from 3 years inside a 24/7 inpatient mental health facility. She lived in an assisted living facility Lenox Hill Hospital, in New York, specifically on a locked “memory care unit” floor. Lenox Hill Hospital, which she was taken to for an independent mental capacity evaluation, forced to stay 3 years. 60 year old former celebrity talk show host Wendy Williams, “claims to be confined to a small area and has only been outside twice in the past 30 days. Williams also states that she eats meals alone in her room because the facility is depressing. She feels suffocated in the “memory unit” where she resides.”
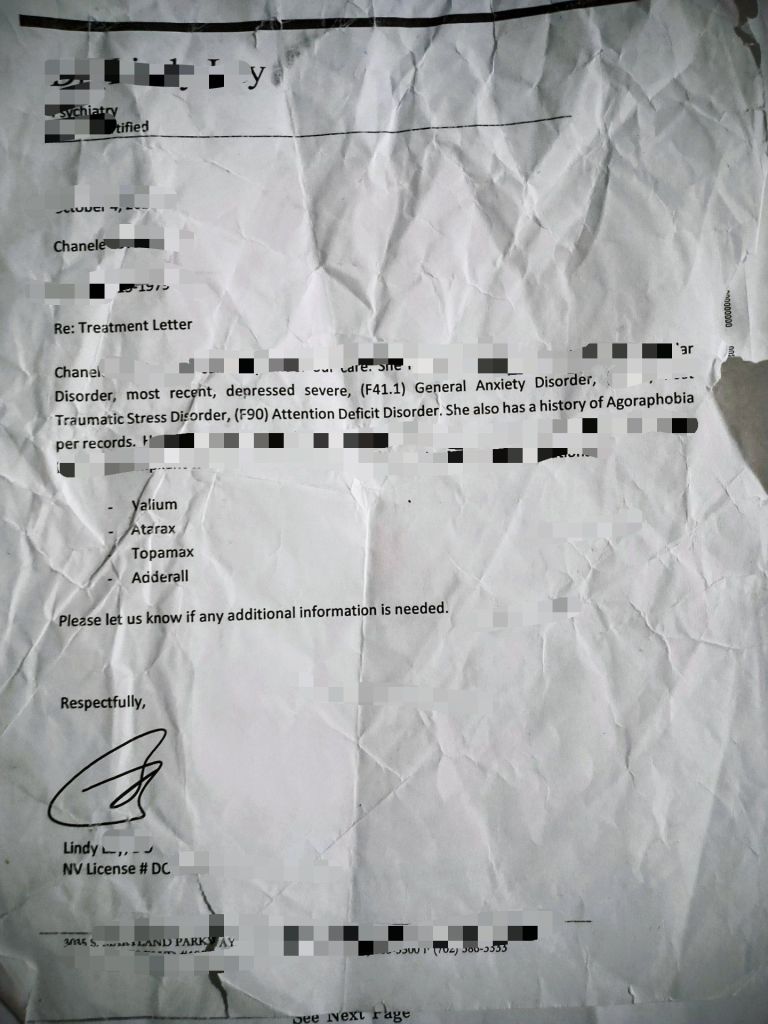
How I attempted to protect myself for years
I can tell you this fear has definitely driven me. For example, this letter below, I used to carry around in my wallet. As you can see from the wear and tear of this digital scan, it has been carried around in my wallet for over 10 years. As well as receiving similar letters from many different therapists, psychiatrists and MDs over the years from the different cities and states I have resided in. People’s words do matter and have many devastating repercussions on both sides of the coin.

I have said all of this prior to getting to informational education, but like Rachel Maddow, I will passionately make my point, when I get there. Before you read my scripted AI driven podcast, I will leave you with this; the perfect world is where everyone would stay out of everyone’s business and mind their own business. However, we know the world can be very ugly and a dismal place at times. We have one game of life so far, in my 46 years on this planet, I have been on a bumpy rollercoaster ride 🥂 Here’s to the next 46 years being in calmer waters. Signing off as Chanele, a real person, a passionate activist, a writer, who informs while entertaining, a loving wife, a courteous neighbor and a compassionate friend, who also happens to be disabled. Do you see a world where that last part doesn’t come with judgement and discrimination? If you do, inbox the DIY version.
Scripted AI driven podcast created by : Ki Lov3 in association with Lov3 books etc. Creative creation edited by: Toni the Editor, DRM (c) October 15, 2025
🎙️The Agoraphobia Myth: Beyond Homebound Stereotypes
When most Americans hear the word “agoraphobia,” a very specific image comes to mind: someone completely homebound, unable to step outside their door, peering anxiously through curtains at a world they can no longer access. It’s a dramatic picture, cinematically compelling, and almost entirely wrong. I’m Dr. Maya Chen, and today we’re going to dismantle one of the most pervasive misconceptions about anxiety disorders in Western society.
Let’s start with the elephant in the room—or rather, the person who supposedly can’t leave the room. Where does this stereotype come from? The answer lies largely in Hollywood’s treatment of the disorder. Think about films like ‘copycat’ from 1995, where Sigourney Weaver plays a psychologist who can’t leave her apartment after a traumatic attack. Or ‘The Woman in the Window’ in 2021, where Amy Adams portrays a reclusive character who literally spies on neighbors from inside her home because she can’t go outside. More examples include ‘Inside’ from 2007 and *Intruders* from 2015—all featuring protagonists who are completely homebound.
These portrayals create what disability rights advocates call the “locked-in narrative.” They’re dramatic, they’re visually striking, but they’re dangerously incomplete. And they have real-world consequences. When employers, family members, or even healthcare providers only understand agoraphobia through this narrow lens, they fail to recognize the vast majority of people living with this condition—people who are struggling, yes, but not in the way movies have taught us to expect.
So let’s talk about what agoraphobia actually is. The American Psychiatric Association made a crucial change in 2013 with the publication of the “DSM-5, the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.” They separated agoraphobia from panic disorder, making it a standalone diagnosis for the first time. Before that, in the DSM-IV, agoraphobia was always tied to panic attacks. This 2013 change was revolutionary because it acknowledged what clinicians had known for years: not everyone with agoraphobia experiences panic disorder. In fact, research shows that approximately 30% of people with agoraphobia don’t have panic disorder at all.
The DSM-5 defines agoraphobia as marked fear or anxiety about at least two of five specific situations: using public transportation, being in open spaces, being in enclosed spaces, standing in line or being in crowds, or being outside the home alone. The key component is that the person fears these situations because escape might be difficult or help might not be available if panic-like symptoms occur.
And here’s where it gets interesting—”panic-like symptoms” doesn’t necessarily mean a full panic attack. It could be fear of losing bladder control, fear of vomiting, fear of fainting, or other embarrassing or incapacitating symptoms. This is far more nuanced than the simple “fear of leaving home” that popular culture has sold us.
Let me give you three real-world clinical examples that illustrate the spectrum of this disorder. First, consider Jennifer, a 34-year-old accountant. She goes to work every day, grocery shops, and attends her daughter’s school events. But she can’t handle enclosed spaces like elevators or theaters. She takes the stairs at work—all seven flights—and sits in aisle seats near exits at any event. She’s not homebound, but her agoraphobia significantly impacts her daily choices and requires constant strategic planning.
Then there’s Marcus, a 42-year-old teacher. He’s perfectly fine in enclosed spaces, but public transportation and crowded areas trigger intense anxiety. He drives everywhere, even 90 minutes to work each way, because buses and trains feel unbearable to him. He grocery shops at 6 a.m. when stores are empty. Again, not homebound, but living with severe limitations that most people never see.
Finally, there’s Diane, 58, who represents the severe end of the spectrum. She hasn’t left her house in two years. She gets groceries delivered and works remotely. She is the Hollywood stereotype—but here’s the critical point: she represents only about 10% of people with agoraphobia. Yet she’s the only version most people know.
This brings us to severity distinctions. The DSM-5 includes specific severity specifiers: mild, moderate, and severe. Someone with mild agoraphobia might avoid one or two situations but still function relatively normally. Moderate means they’re avoiding multiple situations and it’s causing significant life disruption. Severe—like Diane—means the person avoids most or all feared situations and may be completely homebound.
There’s also an important clinical distinction between what doctors might informally call “bouts of agoraphobia” versus “chronic severe agoraphobia.” Bouts might occur during particularly stressful life periods and may wax and wane over time. Chronic severe cases typically require more intensive treatment and more comprehensive accommodations.
Now, let’s talk about something that doesn’t get nearly enough attention in discussions of agoraphobia: the role of privacy invasion as a significant trigger. When someone with agoraphobia—especially those experiencing episodic bouts rather than chronic symptoms—feels their personal space or privacy is violated, it can dramatically exacerbate their symptoms.
This plays out in workplace contexts constantly. Think about someone who’s managing mild to moderate agoraphobia successfully—they’ve found their rhythm, established their coping mechanisms, created their safe spaces. Then their employer installs surveillance cameras, implements invasive monitoring software, or creates an open-office environment where they’re constantly visible. That loss of control over their personal space can trigger an acute bout of symptoms.
Clinically, we understand that agoraphobia is fundamentally about feeling trapped or exposed in situations where escape or help isn’t available. Privacy violations compound that feeling exponentially. If someone already struggles with being observed or judged in public spaces, and then their private spaces—their home office, their personal communications—become subject to scrutiny, it removes their safe zones entirely.
Consider Rachel, a real client case from disability advocacy work. She had what her doctor called “bouts of agoraphobia”—episodic symptoms that she managed successfully. She’d been working from home for a year, her symptoms were stable. Then her company required installation of webcam monitoring software that randomly took screenshots and tracked her activity throughout the day. Within weeks, she couldn’t work at all. Her home—her safe space, the place where she could control her environment and manage her symptoms—had become another place where she felt exposed, watched, and trapped.
This is textbook exacerbation.
The privacy invasion didn’t just stress her out—it fundamentally altered her relationship with her safe environment. For people with bouts of agoraphobia, maintaining control over when and how they’re observed is often critical to their symptom management. When that control is stripped away, even well-managed symptoms can rapidly escalate into acute episodes requiring intensive intervention.
This is where the Americans with Disabilities Act becomes crucial. Agoraphobia qualifies as a disability under the ADA when it substantially limits major life activities. But here’s the problem: when employers, supervisors, and even HR professionals only understand agoraphobia as “completely homebound,” they can’t conceive of what reasonable accommodations actually look like.
Reasonable accommodations are completely individualized based on which situations trigger each person’s symptoms. For someone whose agoraphobia centers on transportation anxiety, accommodations might include remote work during commute hours or adjusted scheduling to avoid rush hour. For someone who struggles with enclosed spaces, it might be permission to use outdoor spaces for phone calls or meetings, workspace modifications to be near exits, or exemption from required elevator use.
For someone with crowded-space triggers, accommodations could include attendance at meetings via video conference rather than in person, flexibility to work during off-hours when offices are less populated, or a private workspace away from open-plan offices. And critically, accommodations around privacy protections—exemptions from certain surveillance measures, private workspaces, or the right to turn off cameras during virtual meetings—aren’t special privileges. They’re necessary protections that allow people with agoraphobia to work without their disability being actively aggravated by workplace policies.
The key point is this: the person with agoraphobia isn’t asking to not work—they’re asking to work differently in ways that accommodate their disability while still fulfilling essential job functions. But we’ve seen discrimination cases where people were denied remote work options or flexible scheduling because supervisors couldn’t conceive of agoraphobia as anything other than complete housebound incapacitation.
The 2013 DSM-5 change helped tremendously with this. By separating agoraphobia from panic disorder, it recognized that agoraphobia is about situational fear, not just panic. This helped legitimize the experiences of people whose agoraphobia manifests differently than the classic “housebound” presentation. It also strengthened ADA claims because it provided clearer diagnostic criteria. Instead of agoraphobia being merely a feature of panic disorder, it became its own recognized condition with specific, measurable criteria. Only a qualified expert in the field is qualified to measure and judge this.
So why does the stereotype persist if it only represents about 10% of cases? The answer is simple: media representation. (As I am known to say, “Representation matters”, and unfortunately our falls short in mass media and entertainment) Movies need drama, and a character who strategically avoids certain situations isn’t as visually compelling as someone who can’t cross their threshold. It makes for good thriller material—the vulnerability is palpable, the dramatic tension is built-in—but it’s like showing only end-stage cancer patients when discussing cancer as a disease. It’s technically accurate for that small subset, but wildly misleading about the condition as a whole.
Here’s what I want you to take away from this: Agoraphobia is a spectrum disorder. Just because someone can leave their house doesn’t mean they’re not struggling. Just because someone needs accommodations doesn’t mean they can’t contribute meaningfully to their workplace or community. And just because you’ve seen a movie about someone with agoraphobia doesn’t mean you understand what the person sitting next to you on the bus might be experiencing.
If you meet someone with agoraphobia, don’t assume you know what they’re experiencing based on a film you watched. Their fears might be specific to situations you’d never expect. Their coping strategies might be invisible to you. They might be the person who always takes the stairs, who always sits near the exit, who shops at odd hours, who works from home not out of preference but out of necessity.
Compassion requires asking and listening, not assuming. It requires understanding that the DSM-5 criteria recognize at least two feared situations from five categories, that severity exists on a spectrum, and that reasonable accommodations under the Americans with Disabilities Act are rights, not favors.⚖️
The locked-in narrative has done immense damage—not just to public understanding, but to real people seeking employment, seeking understanding from family members, seeking accommodations that would allow them to live full lives. It’s time we moved beyond the Hollywood stereotype and into a more accurate, compassionate understanding of this complex disorder.
About 1.5% of the general population lives with agoraphobia. That’s millions of people in the United States alone. And the vast majority of them are not locked inside their homes. They’re navigating a world that wasn’t built with their needs in mind, using strategies most people never notice, and facing a public that’s been taught to only recognize the most extreme presentation of their condition.
We can do better. We must do better. And it starts with understanding that agoraphobia is not a single story—it’s a spectrum of experiences, a range of challenges, and a diversity of needs that require individualized approaches, genuine accommodations, and above all, accurate understanding free from Hollywood’s dramatic but misleading lens.
Until next time, keep questioning what you think you know. Stay tuned for my next episode in this project of being transparent and authentic and getting my say instead of others putting it out in the public putting their spin and narrative.
Episode 2 -” I talk to myself and why?”
Please help 🙏🏾 by
✔️🤑Donating
✔️👍❤️ liking
✔️🫶🙏 Sharing
Donations link 🌐https://hdcgj.betterworld.org/donate
